Dr Sarah Muldoon looks at the conflict many consultants experience in their careers; giving patients the best care and providing meaningful training opportunities.
Search
We've found 316 results
Dr Arun Tohani tells us about his Out-of-Programme Career Break – a once-in-a-lifetime journey to South America, which rejuvenated his spirit and reinforced his commitment to anaesthesia.
The rigorous demands of anaesthetic training in the UK are well known, with long hours, high-stress situations, and the constant need for precision and vigilance. Adding to this the stress of COVID, change in the curriculum, and a wedding to plan led me to look for ways to refresh and rejuvenate myself.
Looking through the Health Education England (HEE) Gold Guide, you can find the information about an Out-of-Programme Career Break (OOPC). OOPCs allow trainees an opportunity to step away from training to give them time to pursue other interests, including interests not connected with medicine. This is different from the other out-of-programme options which are more related to clinical training (OOPT), clinical experience (OPPE) or research (OOPR). This led me down a path I will never regret.
While it's a hugely rewarding and exciting time for any doctor, Dr Tom Walters explores the many challenges of training as a novice anaesthetisit.
A novice anaesthetist will face a range of new environments, technical skills, knowledge, people and equipment. It is easy to feel that ‘the glass is starting to overflow’. However, an understanding of cognitive load theory can be used to optimise complex learning tasks.
It’s beneficial for all anaesthetists to manage cognitive load at work, but also for anaesthetists to implement these principles when teaching in theatre.
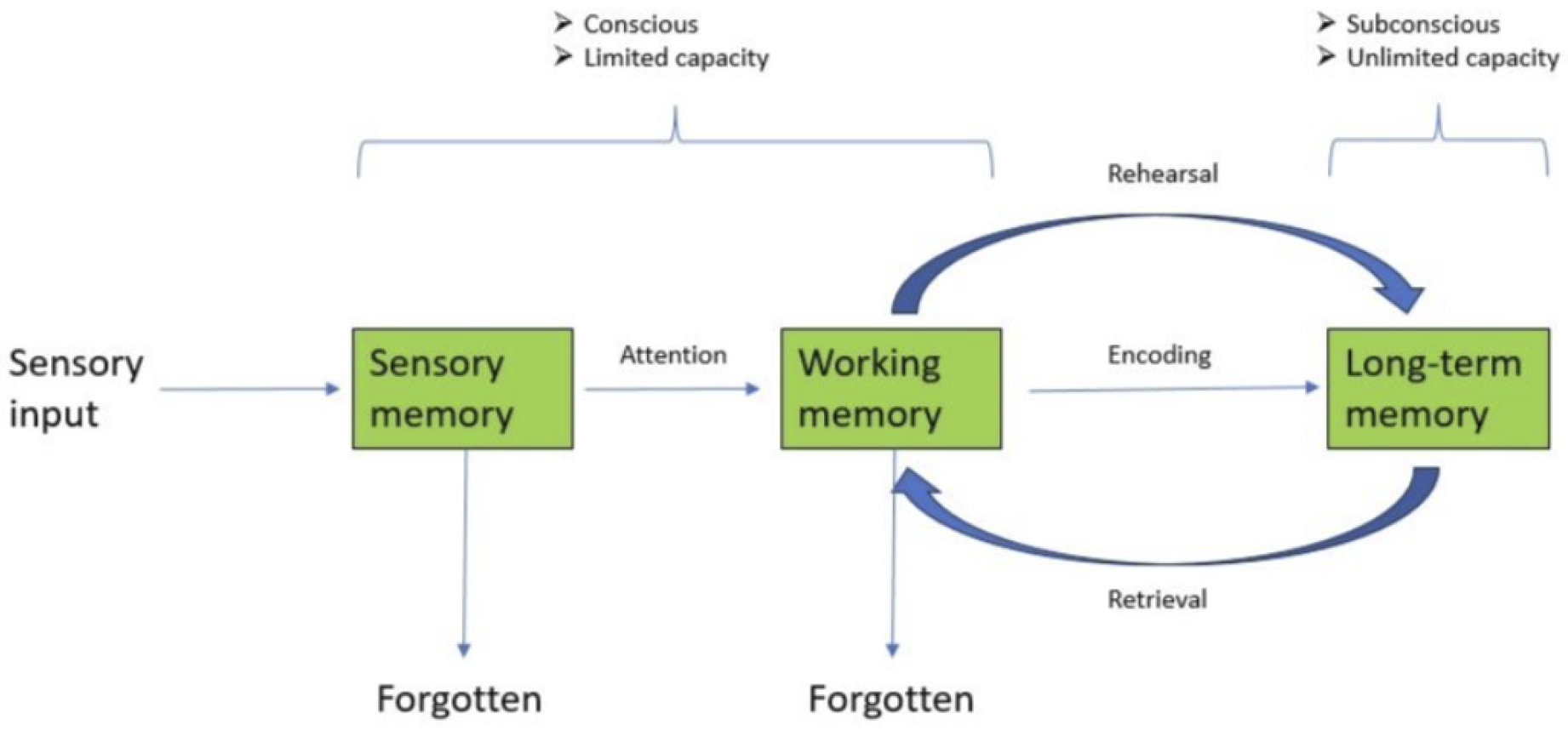
Cognitive load theory has been developed from the Modal model of memory described by Atkinson and Shiffrin. This details how information is received, encoded, stored and retrieved during learning (see An illustration of the Modal model of memory by Dr Thomas Walters). Incoming information is consciously held and processed within working memory, before being encoded into long-term memory. Working memory has a limited capacity, and information within it is transient and forgettable. Once encoded into long-term memory, information is organised in schema, with a seemingly unlimited capacity. Working memory can hold five to nine pieces of information at a time. However, if required to process this information, capacity is significantly reduced.
{kind=link}
Dr Cathryn Malins and Dr Madeleine Storey explain why formalising training time in regional anaesthesia will facilitate the learning of trainees at all stages.
Over the last five years, regional anaesthesia in clinical practice has been on a trajectory – growing in importance and prominence in the anaesthesia community. Efforts by the 8th National Audit Project and the BJA have helped further increase the publicity of regional anaesthesia. While we can all see the merit in this growth, is this the time for a more formalised place in the training programme for regional anaesthesia?
As with any practical procedure, there are many ways to learn, but it is practically impossible to become competent or excellent at regional anaesthesia without regular hands-on patient experience. Recent UK-wide surveys revealed a large proportion of Stage 3 trainees unable to perform all Plan A blocks independently, and found that only a small proportion of consultants and specialists felt confident teaching all these blocks to trainees. It has also been seen that the higher the number of blocks trainees perform, the more confident they feel. Currently, ‘getting numbers’ and achieving the required competence, feels challenging.
We acknowledge that there is an inevitable period of adjustment following curriculum transition, but many of our trainee colleagues still feel their current skills in this area are inadequate for their level of training. To prevent this becoming a perpetual challenge this issue must be proactively addressed across all stages of training.
Dr Chris Carey and Dr Lewis Hendon-John tell us what the College is doing to better understand the factors causing low morale and burnout in anaesthetists.
Training in anaesthesia is one of the cornerstones of the profession. It is often cited as one of the specific attractions of choosing anaesthesia as a career. However, anaesthetists in training are unfortunately not immune from the challenges faced by all resident doctors working within the UK.
In recent years, there have been growing concerns about low morale and burnout. Anaesthetists in training provide a pivotal role in the provision of services in many areas of secondary care. Furthermore, there is a well recognised shortage of consultant anaesthetists in the UK. It’s essential that the NHS is able to train and retain this uniquely skilled workforce to provide care for patients both now and in the future.
It’s apparent from both the College’s own work, such as the 2017 survey on morale and welfare in anaesthetists in training (‘A need to listen’) and also evidence from the GMC’s National Trainee Survey (NTS), that there is a high proportion of anaesthetists in training at risk of burnout. There have also been significant external factors impacting on the training programme, such as the transition to the 2021 curriculum and the COVID-19 pandemic. Competition ratios to enter anaesthetic training are at record levels, and concerns remain about training-post numbers and progression between Core and Higher training programmes.
Dr Tara Keogh looks at how resident doctors can try to implement change and make meaningful contributions while training.
It is not an understatement to say that resident doctors in training often face significant challenges when attempting to implement change initiatives. As they rotate through multiple hospitals, they may struggle to establish rapport and trust with established staff, making it difficult to garner support for new ideas.
The fast-paced environment, heavy workload and burden of exams and portfolio, can leave little time for trainees to engage in the necessary discussions or meetings to advocate for change. Additionally, the hierarchical structure of medical training can inhibit resident doctors from voicing their ideas as they may not feel respected enough to have influence.
‘Safety and Quality Improvement’ is one of the generic professional domains throughout the anaesthetic training programme. Trainees are expected to conduct local quality-improvement projects, in addition to participation in regional or national projects.
Games can be a fantastic way to reset your mind and boost productivity during work breaks. So for this Bulletin issue, we give you the popular Japanese puzzle game, Sudoku.
We've been told playing a game can be a fantastic way to reset your mind and boost productivity during work breaks.
So for this Bulletin issue, we give you the popular Japanese puzzle game, Sudoku.
あなたへの私たちの贈り物 (Our gift to you. Thanks, Google Translate.)
Our full selection of back digital issues has you covered and will keep you up-to-date and informed on what’s happening in our specialty.
Our full selection of back digital issues will keep you up-to-date and informed on what’s happening in our specialty. We hope you continue enjoying your membership magazine.
Find out the latest appointments approved, and with sadness we record the deaths of some of our fellows.
Find out the latest appointments approved, and with sadness we record the deaths of some of our fellows.
Jono Bruun reflects on the work done in 2024 and looks forward to the year ahead.