The History of Anaesthesia
The History of Anaesthesia
“He that sleeps feels not the toothache”
Shakespeare’s observation (from Cymbeline) explains why attempts to alleviate the pain of disease, injury or simple surgical procedures by producing unconsciousness are almost as old as civilization, although the techniques were crude. Most involved ingestion of ethanol and or herbal mixtures, but ‘knock-out’ blows to the head and bilateral carotid artery compression (carotid derives from the Greek for stupor) are also described. These methods were impossible to quantify, and the best that can be said of many is that they were harmlessly ineffective, but that is obviously not the case with head trauma or obstructing the flow of blood to the brain. Hypnotism, introduced as ‘animal magnetism’ or ‘Mesmerism’ in the latter part of the eighteenth century (depicted above), can be effective in susceptible individuals, but such people are relatively rare in developed societies.
Most of the herbal mixtures were devised in Southern Europe or the Orient where plants with active alkaloids (e.g. opium) are indigenous, but one called ‘Dwale’ appears in medieval English texts. Although a number of drugs used in modern anaesthesia have their origins in substances found in plants those early concoctions are irrelevant to the development of effective, drug-induced anaesthesia. It stems from discoveries made in Britain during the latter half of the 18th century, the time of the ‘Enlightenment’. However, di-ethyl ether, the first agent to be demonstrated successfully in public, was originally synthesized (by the action of sulphuric acid on ethanol) in the thirteenth century. There are early reports of it producing both pain relief and loss of consciousness, but such observations were not applied clinically for centuries - examples of a recurring theme: clinical use of the effect did not follow until long after its original observation.
The Discovery and Study of Gases
It was during the Enlightenment that the gases carbon dioxide (Joseph Black, 1754), oxygen (Joseph Priestley, 1771), and nitrous oxide (Priestly again, 1772) were discovered. As with other scientific developments, the therapeutic possibilities were explored and ‘pneumatic medicine’ was born, although many of its practitioners were charlatans happy to defraud a gullible public. However, Thomas Beddoes (once Black’s student) was different, establishing a Pneumatic Institute near Bristol in 1798 to allow objective studies, and appointing the young Humphrey Davy to perform them.
Davy’s ‘Researches, Chemical and Philosophical: Chiefly Concerning Nitrous Oxide’, published in 1799, describes two major effects of its inhalation: euphoria (he coined the term ‘laughing gas’) and analgesia (it eased the pain of his erupting wisdom tooth). Davy suggested inhalation of nitrous oxide during surgical operations, but this was not acted upon (that recurring theme again) though a slightly earlier event may indicate possible explanations. In 1784 a London surgeon, James Moore, published a description of nerve compression in producing numbness for limb surgery – most people have experienced this effect after falling asleep while lying on an arm. The method was used successfully for an amputation performed painlessly by John Hunter, the ‘father’ of modern surgery, yet there is no record of a repeat. Was it fear of complications, inconsistency of effect, or simply that minds were not yet attuned to the concept of surgery without pain?
Davy went on to work at the Royal Institution in London, giving demonstrations of nitrous oxide and other discoveries of the age. In 1813, another scientist famous in later life, Michael Faraday, joined him as assistant and studied the inhalation of ether. He published his findings, which included soporific and analgesic effects, in 1818, but one subject had taken over 24 hours to recover full consciousness. Such an observation provides another explanation for failure to implement important observations – the difficulty of quantifying and controlling their effects.
A much less well-known figure interested in the inhalation of gases is Henry Hill Hickman, a GP from Ludlow in Shropshire, who developed his concept of ‘suspended animation’. This he induced by the inhalation of carbon dioxide, performing operations painlessly on many animals under its influence. Why he chose carbon dioxide rather than nitrous oxide when he was familiar with Davy’s work is one of many unknowns. Hickman’s attempts to publicize his results were unsuccessful, both in England (even Davy was unimpressed) and France, and he died young, but he is the only person in this story to pro-actively conceive of inducing unconsciousness to allow performance of surgical procedures. It is a sign of those times that, while the medical implications of inhaling nitrous oxide and ether were ignored, their potential for ‘recreational’ use was very much taken up: ‘laughing gas parties’ and ‘ether frolics’ were all the rage!
The Great Events
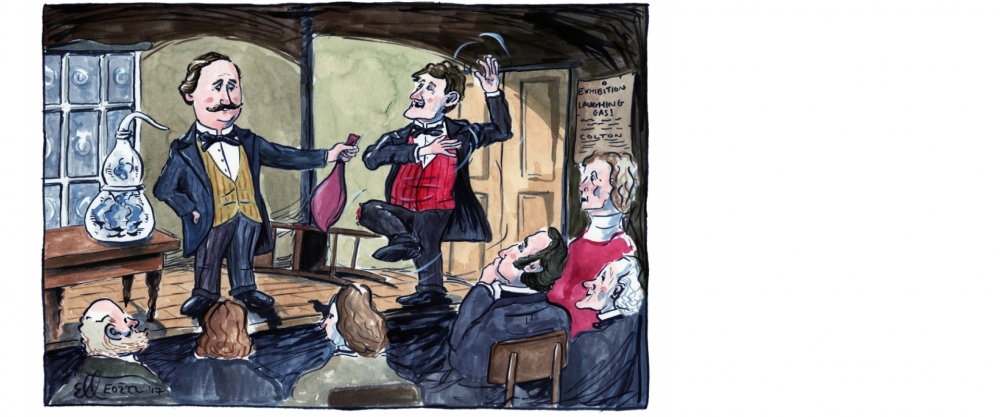
The story moves to the USA, specifically to Hartford, Connecticut on 10 December 1844, when Gardner Quincy Colton, a travelling showman, gave a demonstration of the latest discoveries, including inhalation of nitrous oxide. In the audience was Horace Wells, a local dentist who had mastered the art of using new materials to make dentures, and had sought ways of easing the pain of first removing the patient’s own rotten teeth. Here was a prepared mind, and Wells realized that he might have found a solution when a young man (one Samuel Cooley) who had inhaled the gas injured his shin without any apparent discomfort (note the cut on his knee, and the thoughtful Wells, third from the right).
Discussions led to an experiment the following morning during which Wells had one of his own teeth removed by a colleague, John Riggs, after Colton had administered the gas. Wells learned how to make nitrous oxide, and used it in his practice until he felt confident enough to demonstrate the technique at the nearest major medical centre, Boston. He gave a talk to a class of the Harvard Medical School and then administered the gas to one of them who, unfortunately for Wells, cried out when a tooth was removed. Even though the student remembered nothing Wells reacted badly (he was probably a manic depressive) to being dismissed as a charlatan and, although he continued to use nitrous oxide, he faded from the scene.
However, William Morton, who had previously been both Wells’s student and later partner, had helped with the demonstration, and was made of sterner stuff, recognizing that a ‘better’ agent was required. He was by then a medical student at Harvard and consulted, among others, his chemistry teacher, Dr. Charles Jackson. What part Jackson actually played in Morton’s decision to use ether by inhalation became the subject of great controversy, but there is no doubt that it was Morton who studied it, tested it in animals and then tried it in his patients. Having been successful with these trials he offered to demonstrate his method to Dr. John Warren, surgeon at the Massachusetts General Hospital, and was invited to do so on 16 October 1846. Before a large audience, Morton administered ether vapour to Gilbert Abbott before Warren removed a tumour from Abbott’s neck without any sign of distress. A new era had dawned.

However, unlike Wells Morton was lucky because Abbott was only semi-conscious and remembered events during the operation, but the drug’s effect was sufficient to obtund pain. At first, Morton tried to keep the nature of his agent secret so that he could patent it, but the ethics of the time prevented him from doing so, although scientific credit was hotly disputed. The controversy between Morton and Jackson (later joined by Wells) over primacy raged for so long that the ‘Ether Monument’, commemorating these events in Boston, bears no man’s name, leading it to be nicknamed the ‘Either’ Monument! There is evidence that ether inhalation was used for surgery elsewhere in the USA as early as 1842, but those practitioners did nothing to communicate the news to others, making the events in Boston definitive.
The news spread as fast as the ships of the time could carry it, but that meant that it was December before practitioners in Britain were involved. The first anaesthetics in these islands were given on 19 December 1846, one ‘probable’ in Dumfries (there is no contemporary record) and the other ‘definite’ at 24 Gower Street, London.

Site of the first anaesthetic administered in England
Dr. Francis Boott, an expatriate American, learning of Morton’s success through a letter from Boston, arranged for a Miss Lonsdale to have a tooth removed by James Robinson before a group which included Robert Liston. Liston, then London’s leading surgeon, was so impressed that he arranged to perform an amputation under ether on December 21 at University College Hospital, the first public demonstration in Britain. At the time, James ‘Young’ Simpson, Professor of Midwifery in Edinburgh was on his annual visit to London to learn of the latest advances, and he became an enthusiastic advocate of anaesthesia. He pioneered inhalational analgesia for women in labour, was a major force in countering objections (both religious and medical) regarding its safety and use, and sought a better agent – discovering the anaesthetic properties of chloroform in 1847, the first example of the still continuing search for better drugs and methods.
Major Subsequent Developments
The First Specialists: Thus general anaesthesia was introduced into clinical practice, although objections were to continue for some time, especially after the occasional, perhaps inevitable, death was reported. Inevitable because there was no knowledge of the pharmacology of the drugs, no experience to draw on to guide safe practice, and little understanding of normal physiology, let alone the adverse effects of anaesthesia. All of these problems were compounded by the progressive delegation of administration of the anaesthetic to the more junior members of the surgical team. A very few individuals developed a special interest, notably Dr. John Snow, a London physician, who quickly developed the skills, experience, knowledge and equipment to allow him to publish some of the earliest instructional literature. His reputation grew such that in 1853 he administered chloroform to Queen Victoria for the birth of Prince Leopold, and Princess Beatrice in 1857.
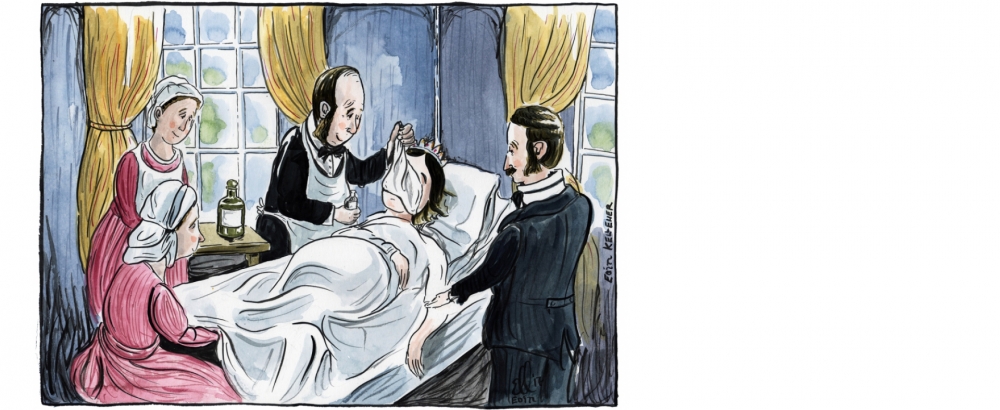
Chloroform a la Reine, note the silk handkerchief from which she is inhaling the vapour!
This royal patronage silenced the last objections to anaesthesia. After Snow’s death Joseph Clover became Britain’s leading specialist, and so these two were chosen as the ‘supporters’ on the College’s crest when the Royal Warrant was obtained.

The supporters either side of the shield on the coat of arms are Snow and Clover
Clover continued to work on control of the concentration of anaesthetic administered, and the monitoring of the unconscious patient. Subsequently, Dr. (later Sir) Benjamin Ward Richardson, who was more scientist than clinician, promoted Snow’s methods, sought better drugs and introduced the ether (later ethyl chloride) spray (see below) for local anaesthesia.
Nitrous Oxide returns: From these historic beginnings the science and practice of anaesthesia grew progressively, the details being beyond the scope of this short account, but a few events require mention. In the USA, Colton continued with his demonstrations, adding mention of Wells’s experiments, such that in 1862 a patient asked him if he would administer nitrous oxide to her for a dental extraction. This he did with such success that Colton gave up his demonstrations and established a company with the specific aim of providing a service for tooth extraction under the effects of the gas. Nitrous oxide, used as the sole agent without oxygen, is safe only for the briefest of procedures, but that made it acceptable for dental extractions, the technique reaching London in 1868.
Clover also found nitrous oxide useful for speeding the induction of anaesthesia with ether, thus starting the trend towards the modern approach of using combinations of several drugs rather than a much larger, and more toxic, dose of one. However, the practicality of nitrous oxide was limited by the need to manufacture it at the site of administration until technical advances allowed it to be stored and transported under pressure in metal cylinders. Here is another explanation for delay between observation and implementation: the necessary equipment had to be developed as well.
Local Anaesthesia: Most of Simpson’s major contributions are noted above, but in 1847 he also suggested that ‘local’ anaesthesia would be even more beneficial than general. Cooling was suggested as a method, and this led Richardson to devise the ether spray, the cooling being produced by rapid evaporation, hence the term still used: ‘freezing’. Pharmacological techniques required recognition of the utility of the ‘numbing’ effects (first noted in 1860) of the South American alkaloid, cocaine. In Vienna in 1884, Sigmund Freud started a study of its systemic effects, assisted by his friend, tyro ophthalmologist Carl Koller. Literal ‘freezing’ is inappropriate to the eye and Koller, who had been taught that a suitable local anaesthetic would be a great advance, had tried the application of several substances without success.
A trainee opthalmologist when he introduced local anaesthesia with cocaine
One day, demonstrating the effect of ‘tasting’ cocaine, he realized that it was what was needed, and trials progressed quickly to clinical use. A paper was read (by a friend, Koller could not afford the trip) at a conference in Heidelberg on 15 September 1884, and this news was around the world in days thanks to the recent introduction of the electric telegraph. Within months most techniques of peripheral nerve block had been described, but greater anatomical knowledge was required before spinal anaesthesia (1898) and epidural block (1921) were developed.
Developments in Surgery: Initially, the introduction of anaesthesia had minimal impact on the scale of surgery, and attempts to increase it ran into a problem: infection. Operations were brief, and mostly minor, until antisepsis and (later) asepsis were developed so that more advanced surgery began to challenge both the skills of the anaesthetists and the quality of their techniques. More sophisticated surgery required more skillful anaesthetists with better equipment and improved drugs; then, once these were available the surgeons increased the challenge again! This cycle has driven progress ever since, with the problems of managing servicemen injured in the two world wars making major contributions to the specialty’s advance.
Muscle relaxation: Another major challenge was surgery to the thorax and abdomen, access requiring relaxation of the muscles of the body wall and diaphragm, an effect needing high concentrations of general anaesthetics. The result is marked depression of circulation and respiration, usually with very delayed recovery of consciousness, the net result being significant morbidity. Once again the solution was in an observation made years before, namely that the South American arrow poison ‘curare’ produces ‘muscle relaxation’ (strictly neuromuscular blockade). Introduced in 1942 by Griffith & Johnson of Montreal, and developed in the UK by Jack Halton of Liverpool, it means that the muscles are relaxed primarily so that the amount of anaesthetic need only be enough to maintain unconsciousness. The method required anaesthetists to learn to insert tubes into the trachea to allow mechanical ventilation of the lung to preserve gas exchange and, consequently, to ‘control’ breathing.
Induced hypotension: In 1948, responding to a surgical colleague’s request for reduced bleeding during vascular procedures, Griffiths & Gillies of Edinburgh described their technique of induced hypotension, the deliberate lowering of blood pressure to achieve that end. This technique has generated more controversy than any other, but the wider implication is that the circulation is as amenable to ‘control’ as breathing.
Subspecialty development: As modern medicine advanced it became apparent that lives could be saved if a patient’s cardiovascular or respiratory failure were to be managed while primary treatment dealt with the underlying disease. Thus the skills learned in the operating theatre were applied to seriously ill patients, and anaesthetists took the lead in the development of intensive care units. 1948 also saw the introduction of the first modern local anaesthetic, lidocaine. The postgraduate examination in anaesthesia, then as now, required knowledge of local as well as general anaesthetic techniques so clinicians were well placed to take advantage of lidocaine’s effectiveness. Skill in nerve block for surgery also has application outside the operating theatre, and so began involvement in the management of acute and chronic pain conditions. To deal with these different aspects of practice the College now has two Faculties: one of Intensive Care Medicine and the other of Pain Medicine.
Postgraduate Training: One consequence of increasing sophistication in anaesthetic techniques is that their benefits will only be obtained if the clinician has the necessary specialist training to implement them safely. As Morton’s example demonstrates, simple ether anaesthesia can be used for minor surgery with little in the way of knowledge, skill or experience. However, multi-drug general anaesthesia involving curare type agents is required for much modern surgery, and would be disastrous in any number of ways if it were not managed properly. The benefits of specialization were recognized very early on, but most early anaesthetists were GPs ‘with an interest’, the general practice side of their work providing their main income.
The consequences of this, in terms of morbidity and mortality, became apparent as techniques evolved during the 1920s and subsequently. The introduction of the first rapidly acting intravenous anaesthetic (thiopental) in 1934 made induction much pleasanter for patients, but its management requires far greater skills than the slower onset of an inhalational agent. Such concerns were behind the major developments in the organizations of the specialty occurring during and after that period. Ensuring patient safety was also behind the establishment, courtesy of Lord Nuffield, of the first academic department of anaesthesia at Oxford under Professor (later Sir) Robert Macintosh in 1937, with the training of others an important function.
Evolution of the Modern Specialty: These many developments all improved the standing of the anaesthetist to that of independent practitioner, a situation confirmed in 1948 by all specialties being given equal status in the NHS. So, by 1950 all of the elements of modern anaesthesia were in place: very few of the drugs of that time are still in use, but their successors are really only improvements on the same theme. Other aspects have changed, and changed hugely for the better with the result that modern anaesthesia has an impressive safety record thanks to two developments. The first is in equipment: the anaesthetist of 1950 (let alone 1850) would gasp in wonder at what is now in daily use.

Compare a modern anaesthetic workstation, above, with John Snow’s silk handkerchief in the earlier picture! The advances include everything from sterile, disposable syringes and needles to computer controlled anaesthetic machines and electronic monitors providing a battery of information on both patient physiology and the proper functioning of the equipment. The second development is even more important – it is in the people required to take advantage of such sophisticated methods. Formal postgraduate training of medically qualified anaesthetists began in 1935 with the institution of the Diploma in Anaesthetics requiring one year’s supervised clinical experience. Today’s Fellowship standard examinations are associated with a competency based training programme of seven years minimum duration. Further, the safe administration of an anaesthetic has long required more than one pair of hands, and the training of those who assist anaesthetists, and the technicians who maintain the equipment, is equally well-defined now.
Sources of Further Information
The above outline barely touches the surface of the history of anaesthesia, but there are many sources of further information, some of the more important being listed below.
Museums, Societies & Websites
There are two major British sources of further information on the history of anaesthesia, both readily accessible:
The Anaesthesia Heritage Centre (www.aagbi.org/education) of the Association of Anaesthetists of Great Britain & Ireland, 21 Portland Place, London W1B 1PY has an important collection of equipment and books. Educational material is available, and there are permanent & special displays.
The History of Anaesthesia Society (www.histansoc.org.uk) has organized one or two meetings a year since it was founded in 1986. The full proceedings, a timeline of anaesthesia and other information are available on the website.
Many medical schools and hospitals have collections, but they are not always generally available. An exception, with a useful website, is:
The Old Operating Theatre Museum and Herb Garret (www.thegarret.org.uk), 9a St Thomas’s St, London SE1 9RY.
General medical and surgical museums often have relevant items as well. In Britain the main ones are:
The Wellcome Collection (www.wellcomecollection.org), 183 Euston Road, London NW1 2BE.
The Hunterian Museum (www.rcseng.ac.uk/library-musems-and-archives), Royal College of Surgeons of England, 35-43 Lincoln’s Inn Fields, London WC2A 3PE.
Surgeons’ Hall Museum (www.museum.rcsed.ac.uk), Royal College of Surgeons of Edinburgh, Nicolson St, Edinburgh EH8 9DW.
The Thackray Medical Museum (www.thackraymedicalmuseum.co.uk), Beckett St, Leeds LS9 7LN
Some important overseas resources are:
The Ether Dome (www.massgeneral.org/history/exhibits/etherdome/), 4th Floor Bullfinch Building, Massachusetts General Hospital, 55 Fruit St, Boston, MA 02114, USA. This, the evocative site of Morton’s demonstration, must be visited if in Boston.
The Wood Library-Museum of Anesthesiology (www.woodlibrarymuseum.org), 520 N. Northwest Highway, Park Ridge, IL 60086-2573, USA
Anesthesia History Association (www.ahahq.org), c/o Dept of Anesthesiology, Vanderbilt University Medical Center, PO Box 128543, Nashville, TN 37232-4245.
The Geoffrey Kaye Museum (http://www.anzca.edu.au/resources/geoffrey-kaye-museum), Australian and New Zealand College of Anaesthetists, ANZCA House, 630 St Kilda Road, Melbourne, Victoria 3004, Australia.
Harry Daly Museum, Australian Society of Anaesthetists, PO Box 6278, North Sydney, NSW 2059, Australia. This site has an extensive ‘Timeline’ of anaesthesia at Online exhibitions – History of Anaesthesia Timeline.
Further reading
Many books have been written on the history of anaesthesia, some of the best appearing during the third quarter of the 20th century, and thus no longer in print. However, copies can be found and are worth the effort:
Keys TE. The History of Surgical Anesthesia. Arguably the best ‘short’ book on the subject; the first edition (1945) was published in the USA by Schuman, and reprinted by the Wood Library-Museum of Park Ridge, USA in 1996. A second, enlarged edition appeared in 1963 from Dover Publications, Inc of New York.
Duncum BM. The Development of Inhalation Anaesthesia. Oxford: Oxford University Press, 1947. This was written for the centenary of Morton’s great demonstration, and was reprinted by the Royal Society of Medicine; copies are available from the History of Anaesthesia Society (www.histansoc.org.uk).
Smith WDA. Under the Influence: A history of Nitrous Oxide and Oxygen Anaesthesia. London: Macmillan, 1982 [ISBN 0 333 31681 9] A compilation of articles published in the British Journal of Anaesthesia between 1960 and 1972.
Davison MHA. The Evolution of Anaesthesia. Altrincham: John Sherratt & Son, 1965.
Sykes WS. Essays on the First Hundred Years of Anaesthesia. Volume 1 – Edinburgh: E & S Livingstone Ltd, 1960; Volume 2 – Edinburgh: E & S Livingstone Ltd, 1961; Volume 3 (Ed Ellis RH) Edinburgh: Churchill Livingstone, 1982
Some more recent publications offer, respectively, a more up to date overview, an indication of how the development of anaesthesia has influenced medicine as a whole, biographies of British academic anaesthetists, and a delightful insight into the eponyms of anaesthesia:
Rushman GB, Davies NJH, Atkinson RS. A Short History of Anaesthesia: The First 150 Years. Oxford: Butterworth-Heinemann, 1996 [ISBN 0 7506 3066 3]
Sykes MK, Bunker J. Anaesthesia and the Practice of Medicine: Historical Perspectives. London: Royal Society of Medicine Press Limited, 2007 [ISBN 978-1-85315-674-8]
Harrison MJ. British Academic Anaesthetists 1950-2000.Wellington: Harrison, 2011 [Volume 1, ISBN 978-0-47320-049-7] & 2015 [Volume 2, ISBN 978-0-473-32137-6]. Also available on-line at http://www.docdr.co.uk/BAA.html.
Maltby JR. Notable Names in Anaesthesia. London: Royal Society of Medicine Press Limited, 2002 [ISBN 1-85315-512-8]
Finally, mention must be made of two major works, one a limited edition publication providing a comprehensive listing of major source documents, and the other an extensive collection of essays, albeit with a North American focus:
Sim P. The Heritage of Anesthesia: An Annotated Bibliography of the Rare Book Collection of the Wood Library-Museum of Anesthesiology. Park Ridge: Wood Library-Museum of Anesthesiology 2012 [ISBN 978-0-9614932-5-7]
Eger EI, Saidman LJ, Westhorpe RN. The Wondrous Story of Anesthesia. New York: Springer, 2014 [ISBN 978-1-4614-8440-0]
Acknowledgements:
Text by Prof Tony Wildsmith, RCoA Honorary College Archivist 2012-15.
Cartoon illustrations provided by Dr Eoin Kelleher.
Picture of Carl Koller used by kind permission of his daughter.
Reproduction of 'The first operation under ether' painting by Robert C Hinckley is by kind permission of The Boston Medical Library in the Francis A. Countway Library of Medicine, Boston.